


|
|
Breast Augmentation Breast augmentation is a surgical procedure to enhance the size and shape of a woman's breasts. This operation has become very popular. In fact, it is the most common cosmetic surgery operation in North America. Last year, over 400,000 women in North America underwent breast augmentation. This number has doubled in the past 5 years. Dr. Peters has been in practice for over 20 years. He has performed breast augmentation surgery on over 4,000 women. In addition, during the past 10 years, he has been the coordinator of a huge, 3,000 patient, international, breast implant research study, involving the reaction of a woman's body to silicone gel breast implants. He has been awarded over $5 million in research grants. He has published over 160 papers and book chapters. He has presented papers at over 300 national and international meetings. For the past 10 years, Dr. Peters has been an advisor to the Food and Drug Administration (FDA), the National Academy of Sciences, the National Cancer Institute, the Institute of Medicine Committee on the "Safety of Breast Implants", and the FDA Public Health Project in Washington, D.C. He is also a member of Health Canada's "Expert Panel on Breast Implants", and Health Canada's "Scientific Advisory Board". He has been a consultant and expert witness in over 35 cases of breast augmentation, throughout Canada and the United States. He has also been a consultant to six major corporations in the United States, with respect to breast implants. Most women requesting this operation feel that, for personal reasons, their breasts are too small. They choose breast augmentation to extend their fashion choices and to improve their self-image. Some patients have always been concerned about their smaller breast size. Others want to "restore" a reduction in breast volume that has resulted following pregnancy and breast-feeding (involution). By inserting breast implants, plastic surgeons are able to increase a woman's bust by one or more cup sizes. The increase in fullness and projection of the breasts improves the balance in a woman's figure and can enhance her self-image and self-confidence. Submuscular versus Subglandular Breast augmentation surgery takes about two hours. An incision is first made. A pocket is then carefully created. The implant is inserted. The pocket is then modified to accommodate the implant. The incision is then closed with sutures. The pocket for the implants can be placed either:
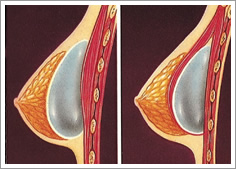 If the nipples are situated above the level of the fold under the breast, and if there is only a minimum amount of breast tissue, then most patients favor placement of the implant under the pectoralis muscle. This tends to give a softer result over the long term.
If the nipples are situated above the level of the fold under the breast, and if there is only a minimum amount of breast tissue, then most patients favor placement of the implant under the pectoralis muscle. This tends to give a softer result over the long term.
However, if the nipples have become lower over time (from pregnancy and breast-feeding), and now rest at or below the level of the breast fold, then there is an advantage to placing the implant on top of the muscle (subglandular). The subglandular placement position lifts low-lying nipples more effectively than the submuscular position. Cohesive Gel versus Saline Implants Today, almost all of women requesting breast augmentation choose cohesive gel implants. Breast implants were originally introduced in 1963. From 1963 until 1992, approximately two million women received breast implants. About 95% of these implants were silicone gel filled. In early 1992, there was considerable controversy about a possible relationship between gel breast implants and certain medical conditions. However, 18 large-scale studies have been conducted over the past decade. They have proven that silicone gel breast implants are not related to any medical condition or disease, even if they should leak. Therefore, in October 2006, Health Canada fully approved the use of cohesive-gel breast implants. They can now be used in any woman who requests them. The main advantage of cohesive gel implants is the prevention of ripples and folds, which can result from saline implants, when there is only a small amount of breast tissue. There are two main types of cohesive gel ‐ soft cohesive gel and firm cohesive gel. Both of these implants are composed of a gel that is much thicker than earlier gel implants. The main advantage of a cohesive gel implant is that if it should ever leak, then the nature of the gel causes it to "e;stick together"e;. This restricts any migration. In addition, the cohesive nature of the gel gives the breast a better shape and texture. Many patients prefer to use the soft cohesive gel, because it feels much softer than the firm cohesive gel. Dr. Peters currently favors Natrelle Inspira Allergen implants and Mentor Elite gel implants. If a woman's chest circumference is narrow, then she may benefit from high profile cohesive gel implants. These have a narrower base and a greater projection than regular implants. The narrow base allows them to sit better if a woman has a narrow chest. Many of our patients choose high‐profile implants. If a woman is particularly slim with a very narrow chest (eg 32 A bra size), then she may well benefit from using Ultra High Profile implants (UHP). These implants have a very narrow base, which allows them to sit better on a smaller chest area (please see "e;patient p"e; in the "e;before and after photos"e;). Under certain conditions, some surgeons may use anatomic or teardrop shaped implants. These probably have little advantage in most women undergoing breast augmentation. In fact, they can have disadvantages. They can shift or rotate, resulting in an altered breast appearance. Similarly, coating the implant with a layer of "e;texturing"e; probably has few advantages in patients. In some, it can have disadvantages, by causing fluid to form around the implant. In others, it can result in wrinkling and palpable edges. Smooth versus Textured Implants Textured implants were initially developed with the hope of reducing capsular contracture, or firmness, in augmented breasts. However, this role has never been proven. About a dozen studies have compared smooth‐surface implants to textured implants. Half of these studies have shown no difference between the two types. The other half have shown conflicting results. The statistical validity of all of these studies has been widely challenged. In addition, most of the studies have been done over only 1‐year, which is a short time frame. Most plastic surgeons continue to use smooth‐surface implants, because of the comparable capsular contracture rates between the two types of implants. They also want to avoid the contour irregularities (wrinkling and palpable edges) that are more common with textured implants. It should be reemphasized that the rate of capsular contracture with all current cohesive gel implants is much lower than with earlier forms of implants. Incisions There are three possible incisions for breast augmentation: 
For patients using cohesive gel implants, we favor the inframammary incision. It usually heals well, resulting in a good quality scar. If the transaxillary (TA) incision is used, then saline implants must be used. They are introduced deflated through the small incision, and then inflated after they are in place. By contrast, the small incision will not permit the insertion of a cohesive gel implant, because it is pre‐filled prior to insertion. It would simply not fit through the small incision. The advantage of the TA incision is that the scar is hidden under the arm. However, there are significant disadvantages with this incision.
|
||||||

|
|
Updated: June 29, 2020 | Copyright © 2020 - All Rights Reserved |
|

